Blog Connection
The Blog connection. Where you can see blogs about Massage therapy and get interesting takes about our industry.
Why I don't buy the idea that "trigger points" are in muscle
Posted by Diane Jacobs
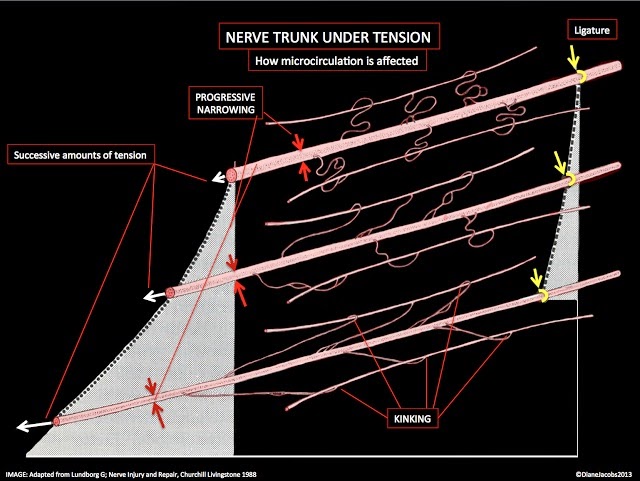
This is what happens when vessels to nerves are under tension
We've all heard of trigger points, right? Those things that hurt when you press on them or when someone else presses on them. Right? So far, so good. They are spots, or points, fair enough; and they hurt when provoked, i.e., they "trigger" discomfort. I can accept all this so far. We have something physical, a sore spot, and we have some action, provocation that makes said spot hurt.
It all gets rather smushed together, this (ectodermal) phenomenon called "pain" being generated somehow, then "felt" or perceived as being associated with some (mesodermal) part of the body, with a motor deficit or malfunction of some sort, such that when a certain movement is attempted it is thwarted by a pain signal. I suspect it was the interference with motor output that made it somehow acceptable to leap to the conclusion that muscle was somehow to blame. But it isn't, not necessarily. Correlation is not causation. After all, muscle is just doing whatever the CNS tells it to do. Really. Muscle is just a puppet of the nervous system. It has no "behaviour" other than doing whatever the nervous system decides it needs (non-conscious) or wants (conscious) to do.
Now, why in the first place trigger points were ever blamed on muscle is probably, in retrospect, just sloppy, convenient, heuristic thinking. I can accept that stuff like that goes on all the time. Why such sloppy, convenient and heuristic thinking is allowed to continue when better explanations have come to exist, I don't understand, and sort of resent actually..
THE ANATOMY
First of all, supposed "trigger points" are found/discerned/their existence implied from outside a patient by another person poking at them. Let's bear in mind that there is a thick layer of blubber, even on skinny people, between a patient's "muscle" and a practitioner's finger poke. Let us not automatically mentally subtract the outer layer as inconsequential, the way trigger point diagrams would have us do.
That layer, known as cutis/subcutis, usually a good half inch thick, contains:
1. a huge amount of neural structure, i.e.
- Cutaneous nerves with all their rami to the surface
- All the neural receptors needed to signal the state of the environment to the brain
- All the neural structure required to regulate blood flow in the skin organ which according to Gray's Anatomy, is ten times that required to maintain the skin organ itself.
2. a huge amount of vascular structure, for thermodynamic radiation of heat away from person-as-organism
3. Plenty of smooth muscle tissue, responding not to the will of a person but rather to brainstem exigencies/dictates, e.g. shivering/goosebumps, vascular lumen contraction via sympathetics, vascular lumen enlargement via efferent neuropeptide leakage by afferent sensory neurons, plenty of opportunity for nociceptive afferents to be bothered by sympathetic efferents and vice versa.
Could it be, therefore, that "trigger points" are no more than areas of secondary hyperalgesia? Tell me how it is possible to diagnose "trigger points" in striated muscle, through a half inch of protective cutis subcutis full of all sorts of autonomic behaviour and potential afferent crankiness, plus a dense layer or two of fascial containment around said muscle? I just don't buy it. And I can't buy any diagram that shows red striped muscle with a red "x" on it, indicating a sore spot, with no skin over it or neural structure depicted in the area. I.e., Travell and Simons. To me, all this blaming a muscle for pain is a good example of looking backward through a telescope. It can be done, I suppose, but it doesn't help anyone see or conceptualize anything better. (I realize this all sounds like heresy. So shoot me. But please read on.)
FAULTY REASONING
Several years ago, Quintner and Cohen pointed out some of the logical problems inherent in the 'myofascial' idea surrounding the phenomena of "trigger points", making what I still think is a really good stab at deconstructing the nonsense in which they (still) remain embedded. See their article, "Referred Pain of Peripheral Nerve Origin: an Alternative to the "Myofascial Pain" Construct." I think it's a great article, one of a kind, but still, I wish they had gone further and pointed out or at least mentioned that no tissue other than neural tissue (i.e., neurons, direct ectodermal derivatives) can directly signal the brain (also direct ectodermal derivative) to provoke it into mounting a pain output/perception for our conscious awareness to,.. um, be aware of, consider. In other words, quite apart from the "trigger point" issue, is there really any such thing as "myofascial pain"? I would argue that no, there isn't. Only neural tissue can send sensory-discriminative information to the brain, and only the brain can mount that sort of cognitive-evaluative-motivational-affective-sensory-discriminative display known as "pain". Other kinds of tissue in the body are usually innocent victims, not guilty culprits. (I can hear people thinking, "But what about inflammation? The immune system?" Yes, the immune system can bother the nervous system, terribly, but ultimately, the internal regulation system controls the immune system, so there you go. The only exception I can think of is a channelopathy or other genetic or epigenetic pathology. For regular garden-variety mechanical pain? Not so much. Please read on.)
ALTERNATE EXPLANATIONS THAT MAKE WAY MORE SENSE
A few years ago I started reading about tunnel syndromes. There are more than enough of these described in this book (see below) that I think I'll go with the idea that most of the "pain" (in the mechanical sense) experienced as being located in the body, is likely due to one or more neural entrapments, not misbehaving mesoderm being some sort of causal factor.
TUNNEL SYNDROMES
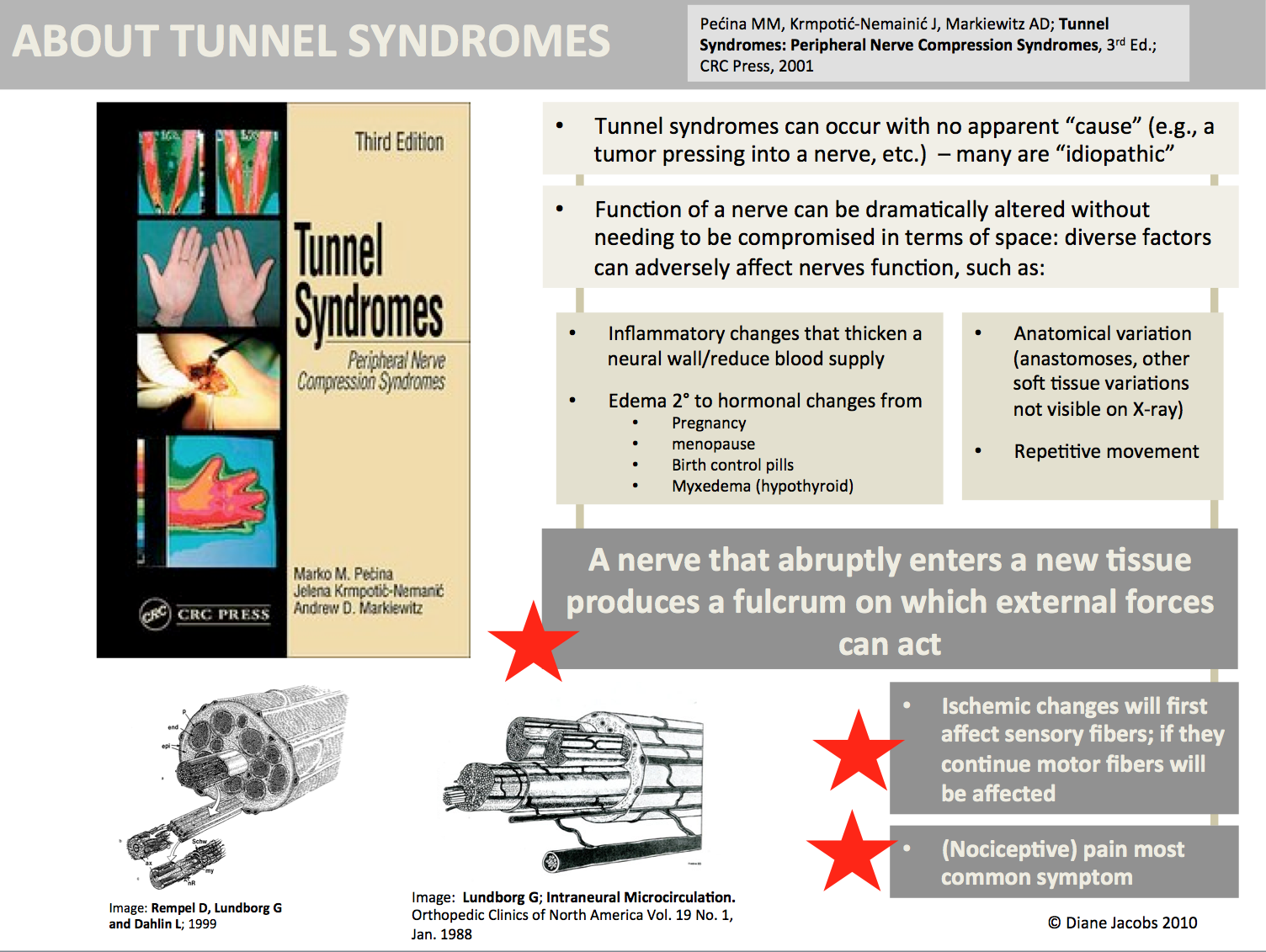
In the book, Tunnel Syndromes, (Marko M. Pecina , Andrew D. Markiewitz , Jelena Krmpotic-Nemanic, 2001) over 50 different neural tunnel syndromes are described and illustrated. The non-invasive treatment recommended in this book is kinda pathetic, really, but they probably don't realize what manual therapy can do with mechanical pain, and each tunnel syndrome is fully described and its diagnosis differentiated. Here is what the authors say:
1. Tunnel syndromes can occur with no apparent “cause” (e.g., a tumor pressing into a nerve, etc.) - many are “idiopathic”
2. Function of a nerve can be dramatically altered without needing to be compromised in terms of space: diverse factors can adversely affect nerves function, such as:
- inflammatory changes that thicken a neural wall/reduce blood supply,
- edema 2° to hormonal changes from pregnancy, menopause, birth control pills, myxedema from hypothyroidism,
- anatomical variation (anastomoses, other soft tissue variations not visible on x-ray), or
- repetitive movement.
3. A nerve that abruptly enters a new tissue produces a fulcrum on which external forces can act.
4. Ischemic changes will first affect sensory fibers; if they continue motor fibers will be affected.
5. Pain (i.e., nociceptive input, nociception) is the most common symptom.
(I would add, pain on provocation, or secondary hyperalgesia, fits in here too, since nerves themselves
a) can "hurt" because of being innervated by nervi nervorum, and
b) come all the way out to skin by way of cutaneous rami sheathed in skin ligaments.)
NEURODYNAMICS
So, in addition to repetitive movement, how about not enough movement, or variety of movement?
I would urge everyone to get a copy of Rempel D, Lundborg G, Dahlin L;
Pathophysiology of nerve compression syndromes: response of peripheral nerves to loading.
J Bone Joint Surg Am. 1999;81:1600-10.
Check out the wonderful diagram of the microanatomy of peripheral nerve it contains (posted above).
Lundborg, back in the 80's, worked out the microanatomy, how the vascular supply inside a nerve worked, what assisted it to function (um, movement), what happened to it if it became impaired, the sorts of mini-compartment syndrome effect this could have; he measured all sorts of finicky pressure gradients within a given nerve, and so on. Without lymphatics (although this idea of no lymphatics inside nerves is itself disputed by some), sometimes venous drainage alone can't take care of all the neural needs by itself, in there. Inside a tunnel. Who needs to worry about external compression on a nerve if it can develop problems all on its own inside its own tunnel? From blood flow backed up? I.e., increased volume? Lately Coderre has hypothesized a link between mini-compartment syndrome of blood flow in nerves and CRPS.
Why did Lundborg bother studying all this nerve stuff? Because he was learning how to do nerve grafts, and was trying to figure out what he had to do to keep his grafts from failing. What must have been blatantly obvious to him was that nerves have/are special kind of tissue(s) and require just the right conditions to grow together again.
Why should we as manual therapists care about any of this? Because by knowing about it, by knowing about nerves and the kinds of trouble they can get themselves into, how they can become nociceptive "drivers" themselves, we can drop off a lot of cumbersome and useless hypothetical baggage that forces us to consider and develop extraneous ideas about what tissue we think we are treating when we treat "trigger point" "pain" in people.
If we can get onto the correct tissue conceptually, then we stand a better chance of getting on the right tissue perceptually, too.
As always, it doesn't hurt to remember that the nervous system is only 2% of the body but uses up 20% of available energy, signals itself constantly at an average speed of 120 meters per second, constitutes 72 kilometers of nerve in a single human, and if every neuron were laid end to end, it would be more like 100,000 km.; that if a neuron's soma were the size of a tennis ball, its axon would be a half mile long and the size of a garden hose. The other 98% of the tissue comprising the human body doesn't know, doesn't much care, lives fast, dies young, replaces itself without much fuss. In other words, don't blame mesodermal derivatives for things over which they have absolutely no control. They're just passing through something called a human life, controlled for the length of a life span by something called a nervous system. Treat that instead - it can respond to what you do. From skin cell to sense of self. Continuous and indivisible from a signalling point of view. The other stuff can't.

|
|
|
Two different sources on tunnel syndromes, same information re: mechanism |